どうも、こんにちは。ミネルヴァのフクロウです。メンタルに関する活動をしながら、日々の活動を通じて皆様の心の健康に役立ちそうな情報を発信しています。
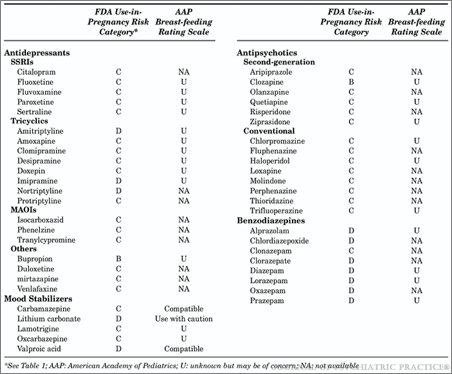
The use of psychotropic medications in pregnancy
Background risks
The spontaneous abortion rate in confirmed early pregnancy is
10–20% and the risk of spontaneous major malformation is 2–3%
(approximately 1 in 40 pregnancies).
• Smoking, poor diet and drinking alcohol during pregnancy can
have adverse consequences for the foetus.
• Moderate maternal caffeine consumption may be associated with
low birth weight.
• Pre-pregnancy obesity increases the risk of neural tube defects
• Psychiatric illness during pregnancy is an independent risk factor
for congenital malformations and peri-natal mortality.
• Affective illness increases the risk of pre-term delivery.
Effect of medicines
• Drugs account for a very small proportion of abnormalities (approximately
5% of the total). Potential risks of drugs include
– major malformation (first-trimester exposure)
– neonatal toxicity (third-trimester exposure)
– longer-term neurobehavioural effects and increased risk of physical
health problems in adult life.
• The safety of psychotropics in pregnancy cannot be clearly established
because robust, prospective trials are obviously unethical
– We rely on database studies, prospective data from teratology
information centres and published case reports. At worst there may be
no human data at all, only animal data from early preclinical studies.
• The patient’s view of risks and benefits will have paramount importance.
General principles of prescribing in pregnancy
In all women of child bearing potential
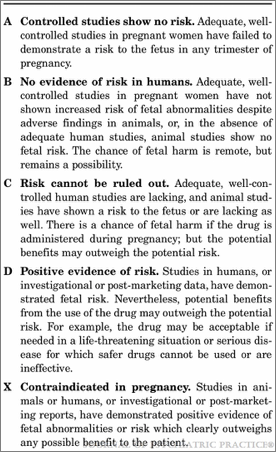
• Try to avoid drugs that are contra-indicated during pregnancy (especially valproate and carbamazepine).
If prescribed, women should be made fully aware of teratogenic potential. Consider prescribing folate
If mental illness is newly diagnosed in a pregnant woman
• Try to avoid all drugs in the first trimester (when major organs are being formed)
• If non-drug treatments are not effective/appropriate, use an established drug at the lowest effective dose
If a woman taking psychotopic drugs is planning a pregnancy
• Consider discontinuing treatment if the woman is well and at low risk of relapse.
• Discontinuation of treatment for women with SMI and at a high risk of relapse is unwise, but switching to a
low risk drug may be appropriate.
If a woman taking psychotropic medication discovers that she is pregnant
• Abrupt discontinuation of treatment in women with SMI and at a high risk of relapse is unwise;
• Consider remaining with current (effective) medication rather than switching, to minimise the number of
drugs to which the foetus is exposed
In all pregnant women
• Ensure that the parents are as involved as possible in all decisions
• Use the lowest effective dose of the drug with the lowest known risk to mother and foetus
• Prescribe as few drugs as possible both simultaneously and in sequence
• Consider referral to specialist peri-natal services
• Ensure adequate foetal screening
• Be aware of potential problems with individual drugs around the time of delivery
• Inform the obstetric team of psychotropic use and possible complications

コメント